Classical anatomy defined the skin as the “involucrum corporis humani”, or the envelope of the human body. This concept expressed the frontier status of the skin and its role as the organ of exposure.
the skin
the main barrier
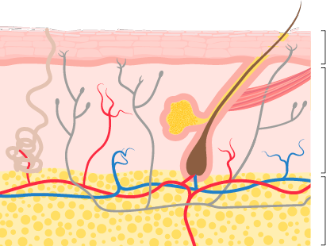
The skin constitutes the largest organ in the human body, with a surface area of nearly 2m² and a weight that represents approximately 6% of total body weight.
The skin separates the external environment from the body’s internal environment, but this separation is not isolating, because interchanges take place between external agents and the bodily functions that contribute to shaping the appearance of the skin.
1
2
3
4
5
6
blood vessels
1. Blood vessels
The blood vessels of the dermis are fine capillaries that come from the medium-sized vessels of the hypodermis.
The blood vessel network of the dermis not only supplies oxygen and nutrients to the cells and the structures located in this layer, but also nourish the cells of the epidermal layer that lacks blood vessels.
The dermis performs a fundamental role in the regulation of body temperature, in which the blood vessels and sweat glands participate.
innervation of the skin
2. Innervation of the skin
Two types of nerve fiber can be found in the dermis:
The motor nerves:innervate the blood vessels,
the glands and the hair erector muscle. The sensory nerves: are
free or encapsulated nerve endings that act as heat, touch and pain sensory
receptors.
The stimuli received by the skin’s surface are captured by the receptors of the dermal nerve endings, that transmit this information to the brain, which returns it processed in the form of a response
skin appendages
3. Skin appendages
The skin appendages are epidermal formation of the skin. There
are three different groups:
Pilosebaceous unit: an anatomical and functional unit consisting of the hair and its appendages; sebaceous gland, apocrine sweat gland and arrector pili muscle. The apocrine sweat
gland. The nail
epidermis
4. Epidermis
Structure responsible for protecting the body from external
agents:
Physical: solar radiations, injuries,
etc. Chemical: penetration of
substances. Biological: pathogens (bacteria, fungi, etc.).
Protective function against the loss of water, preventing the
dehydration of the skin by:
Keratin formation or keratinization. Melanin synthesis or
melanizatio.
dermis
5. Dermis
Its function is to give the skin strength and elasticity. Blood and lymphatic vessels run through it, the skin appendages are found within it, as are the sensitive receptors of the skin. Formed by connective tissue, it is comprised of:
Skin cells: Fibroblasts, histiocytes, mast cells, capable of engulfing and developing a response against foreign agents, protecting the dermis against microorganisms.
Dermal fibers: collagen, elastic and reticular, they make up 90% of the structure of the dermis.
hypodermis
6. Hypodermis
Variant of the connective tissue that is known as adipose tissue. The abundance of subcutaneous fat tissue varies depending on the area of the body, gender and nutritional status, and there are two groups: Android (typical of men) and gynecoid (typical of women)
Main functions Protective: cushions
impacts, shocks, etc. Metabolic: the adipose panicle is a store
of energy. Plastic: the hypodermic adipose tissue shapes the
figure. Thermoregulatory:the fat acts as thermal insulation.
Skin aging is a gradual process perceived by changes in the appearance and texture of the skin.
These changes are a consequence of the passing of time (chronoaging or intrinsic aging), exposure to solar radiation (photoaging), lifestyle and other environmental or external factors. Thus, skin aging does not always match the chronological age, but reflects the skin’s biological age.
According to the aging scientific approach defined by dr. Glogau, skin aging can be classified in 4 degrees that gradually reflect the intensity of the epidermal and dermal damage.
The 4 degrees of aging should be treated differently and gradually.
STAGE I
STAGE II
STAGE III
STAGE IV
STAGE I:
Modifications
Increase in oxidative processes and the action of free radicals.
Increase in the loss of transepidermal water and reduction of amino acid and protein levels.
Weakening of the cell barrier.
Consequences
Increase in skin opacity.
First expression lines.
Fine wrinkles.
STAGE II:
Modifications
Reduction in the capacity of fibroblasts synthtesis, that results in a reduction of collagen fibres and elastin levels.
Reduction in the quantity and quality of the skin structural elements which are part of the support structure of the dermis (fundamental substance).
Consequences
Reduction of the dermis thickness that results in a loss of skin firmness.
Increase of deeper wrinkles.
STAGE III:
Modifications
Reduction of the number of cells in a maturation stage which are the responsibles of the skin structures (slowing down of cell renewal).
Loss of efficacy of the metabolic processes which influences in the normal skin deterioration.
Deterioration of the external epidermis layers and reduction of the quality of the skin support tissue.
Consequences
Gradual decrease of skin elasticity together with lack of firmness.
Deep wrinkles.
STAGE IV:
Modifications
Destructuring of intercellular junctions of the external skin layers.
Reduction and loss of metabolic function of the oil and sweat glands.
Hyperkeratination of the stratum corneum (rough to touch).
Consequences
Loss of definition of the facial contour.
Increase in skin fragility.
Very deep wrinkles.
pigmentation
alterations of pigmentation
MELASMA
PIH
SOLAR LENTIGINES
SENILE LENTIGO
EPHELIDES
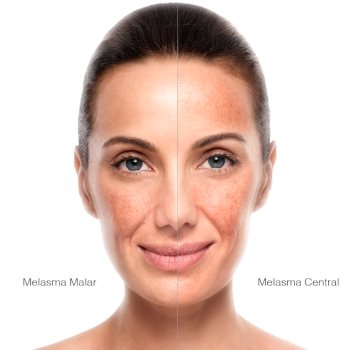
Melasma:
Melasma or cloasma is an acquired hypermelanosis that manifests in areas exposed to the sun, particularly the face. They are dark brown spots, extensive, irregular in shape that appear on the face, forehead and upper lip. They appear due to hormonal changes that stimulate the melanocytes.
The usually appear in pregnant women, users of
OCPs and menopausal women. This alteration is made worse by the sun.
There are two types:
Midface: forehead, nose, chin, upper lip and center
of the cheeks.
Malar: cheeks and nose
PIH:
Post-inflammatory pigmentation (PIH) causes darkening of the skin. It takes the form of different-sized spots. PIH is caused by an increase in melanin synthesis in response to an inflammatory injury or damage to the skin.
If the excess melanin is produced on the top layer of the skin (epidermis) the hyperpigmentation is brownish in hue.
If the excess melanin is produced in the lower layer of the skin (dermis) then it acquires a gray-blue coloration
Although PIH can occur in every skin type, it is most common in the
higher phototypes V and VI and can affect both men and women equally.
Solar Lentigines:
Solar lentigines are spots on the skin associated with aging and exposure to ultraviolet radiation from the sun. They vary in colour, from light brown to red or even black, and are located in the areas most exposed to the sun, particularly the hands, face, shoulders, arms and forehead, even the head if it is hairless.
From the age of 40, the skin starts to lose its ability to regenerate and recover from exposure to the sun, and the solar lentigines are very common in this age range, especially in those who spend time exposed to the sun’s rays.
Senile Lentigo:
Senile lentigines are brown to dark brown coloured macules, from a few millimetres to 1-2 cm in diameter. Their surface is smooth and well defined. They usually appear after the age of 40 due to the cumulative effect of the sun and because with age melanin is unevenly distributed in the epidermis.
They are more frequent in the areas exposed to the sun like the face, back of the hands and neckline. They appear as flat, brown coloured spots, and are predominantly oval in shape.
Ephelides:
Ephelides are a congenital alteration of the pigmentation that are revealed by exposure to the sun. They are commonly called freckles.
They are macules of a few millimetres diameter, light yellow or light brown, which usually appear in people with red hair or blondes with light-coloured eyes. Their number increases with age
They are located mainly on the face, neck, forearms and legs, covering the shoulders, arms and thighs during the summertime.
sensitive skin
circulatory alterations
Microcirculation is the circuit used by the organism to transport nutrients to the tissues and to eliminate cell debris and waste substances.
Fragility, a tendency to redden and suffer irritations and above all the possibility of developing hyperactivity are characteristics of sensitive skins. They are due to alterations in the barrier function, which produces a special sensitivity of the epidermis to stimuli that can be classified into two groups:
- External stimuli: the climate, light, cosmetics, pollution, etc.
- Internal stimuli, such as stress, individual conditions, tiredness, etc.
ERYTHEMA
ERYTHROSIS
COUPEROSIS
ROSACEA
Erythema:
Erythema is a reddening of the skin due to an excess blood supply
produced by vasodilation; it is a symptom of different skin conditions;
it is usually the most visible sign of a skin process that determines
its size.
We may come across two types of erythema:
Solar erythema (induced), with
the symptoms:
Reddened skin caused by sun exposure.
More visible in phototypes I, II.
Vasodilation.
Blushing (spontaneous), with the symptoms:
Reddening of the cheeks
Localized vasodilation
Stimulation of the nerve endings
Erythrosis:
This is reddening of the face (mainly the midface
area). Its origin is a slowdown of the venous circulation.
The triggers can be hot drinks or food, the
changes in temperature or emotions. At first it is transient, but with
time the redness becomes permanent.
Couperosis:
Couperosis is an alteration of the vascularization
of the dermis of the face and neckline which is expressed in the onset
of redness. It corresponds to a network of telangiectasia on a
background of erythrosis.
It is more common in skins that are thin, white,
sensitive and pallid, which redden easily because their epidermis is
very thin. The elasticity of these peripheral vessels is virtually zero.
If the blood flow suddenly increases and the capacity for elastic
recovery is scarce, this redness may easily occur.
The formation of couperosis is influenced by
external factors (chemical agents, contusions, environmental exposure)
and internal ones (digestive disorders, nervousness, stress,...).
Rosacea:
Rosacea is a vascular disease of the face that appears as a consequence
of a long evolution in four stages:
Erythema
Erythrosis
Couperosis
Rosacea
This condition can be confused with and in some cases coexist with acne
vulgaris and/or seborrheic dermatitis.
Rosacea affects both sexes, but is almost three times more common in
women (high incidence during the menopause) and has a developmental age
between 20 and 60 years of age.
The presence of reddening in the scalp or ears suggests a different
diagnosis or other concomitant conditions, since rosacea is
predominantly facial.
acne
oily skin and acne
Acne is a condition with a very high incidence. Between 80% and 90% of the population suffer
from it during their lifetime, the incidence among people between ages 12 to 18 is 74%.
It is caused by an excess of androgen and is the result of different trigger factors. It is
characterized by a polymorphic skin condition with various types of lesion. The main factors
are: excess of sebaceous secretion, reaction to the normal bacteria found on the skin,
obstruction of the pilosebaceous unit.
According to the degree of development, it can have psychological and social implications,
that worsen the quality of life.
MILD
MODERATE
SEVERE
VERY SEVERE
Mild:
Comedones and papules
Moderate:
Comedones, papules and some pustules.
Severe:
Comedones, papules, pustules and some nodules.
Very severe:
Comedones, papules, pustules, nodules and scars.
skin type
DRY
NORMAL
OILY
Physiological characteristics:
Insufficient sebaceous secretion and/or dehydration of the stratum corneum.
It is especially common in women.
Causes: inherent in the person or due to external factors, which alter the skin barrier.
Integrity of the stratum corneum.
Visual inspection:
Matt, shrivelled appearance.
Tendency to redness and peeling given its vulnerability to external agents.
Pores barely or not discernible.
Peeling in areas.
Tactile inspection:
Rough to the touch. Elastic and flexible.
On palpation, the skin fold feels relatively thin as evidence of a fine skin.
Properties:
The lack of protection leads to dehydration.
Poorly withstands the extremes of weather: cold, wind, etc.
Poorly tolerates soaps, detergents, antiseptics, etc.
Tans reddening or does not tan.
Physiological characteristics:
Adequate sebaceous secretion.
Well-hydrated stratum corneum.
Balanced secretions.
Integrity of the stratum corneum.
Visual inspection:
Moderate gloss, matte.
Uniform color.
Overall appearance fresh, luminous.
Pores not visible to the naked eye.
Tactile inspection:
Smooth, with fine graininess..
Elastic and flexible.
Properties:
Soaps are well tolerated due to its buffering capacity.
Tans moderately in the sun.
Resists climatic factors.
Reacts rapidly to the pinch test.
Physiological characteristics:
Increase of the secretory activity of the sebaceous glands.
Frequent between the ages of 15 and 20, both in men and women.
It is usually accompanied by keratosis.
At times of excess sweating.
Visual inspection:
Greasy shine, particularly in the midface region.
Midface zone is more thickened: diffuse and perifollicular hyperkeratosis; the pore is
sinking and clearly visible.
Pore visible.
Does not normally exhibit redness, peeling.
Tactile inspection:
To the touch it has a granular feel, although smooth and oily.
On palpation a thick skin fold is noted as a consequence of the increase in volume and
the hyperactivity of the sebaceous glands.
Properties:
Strong defensive capability.
Strong resilience.
Resists aging very well.
Resists the sun well, good pigmentation, without sunburn.